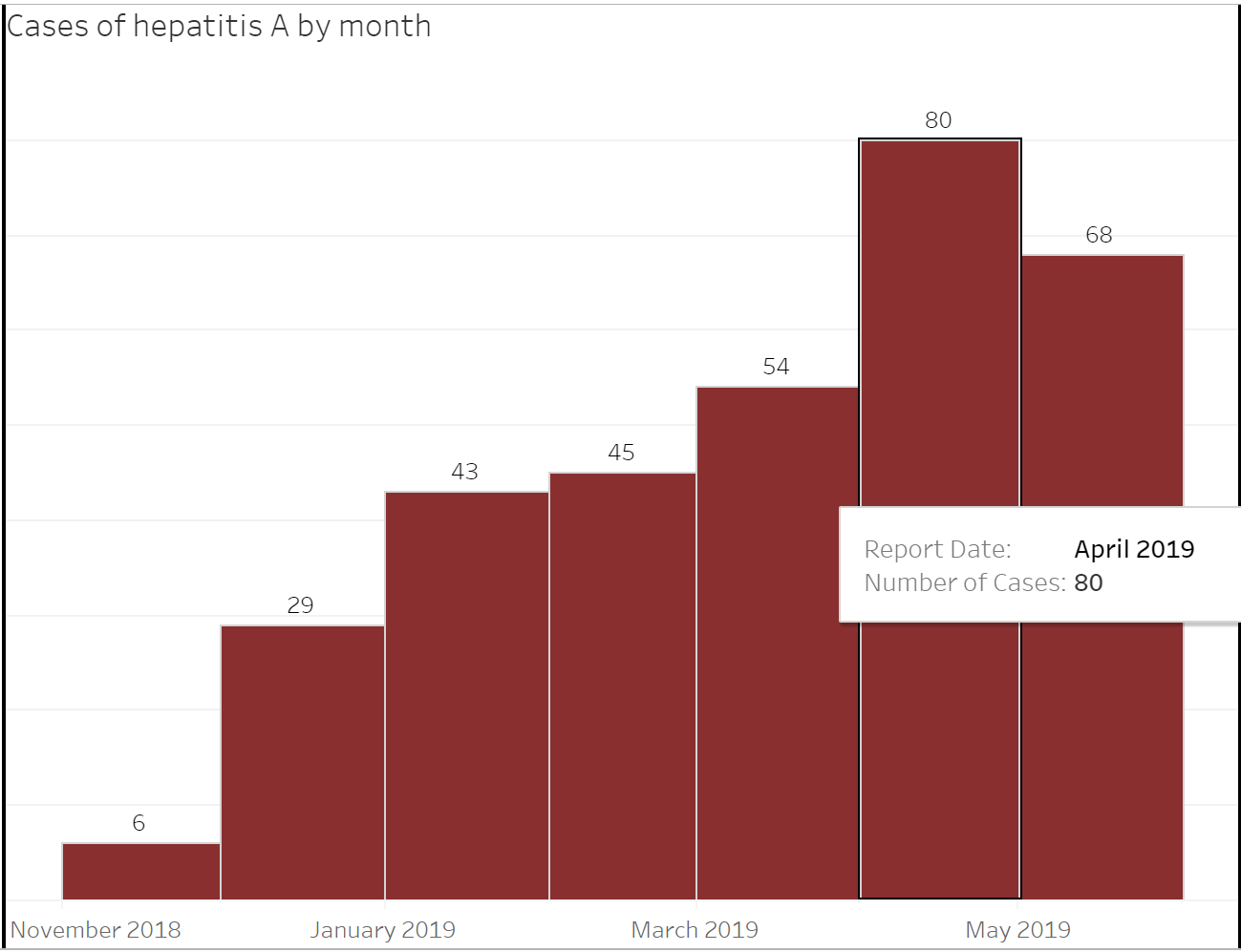
Hepatitis A Outbreak Dashboard and Resources are Live
We recently launched an interactive dashboard and a number of resources to support the hepatitis A outbreak response efforts of county and tribal health departments, health care providers, and correctional facilities in Arizona. Tracking when and where the outbreak is occurring and who it is affecting is critical to the response. There have been more [...]



Social Media