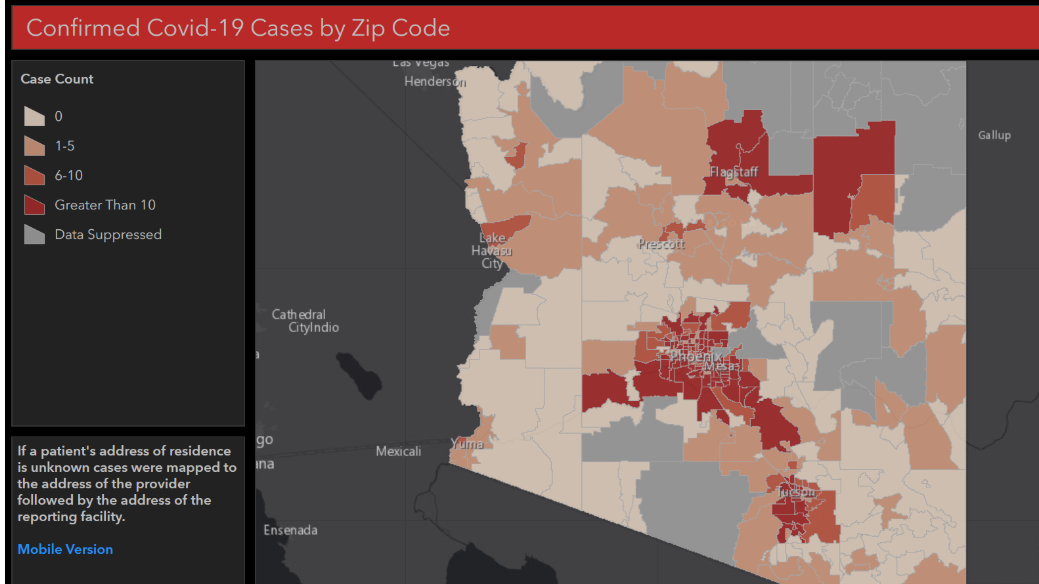
New COVID-19 Data Released on our Dashboard
Today we added data to our COVID-19 dashboard that includes additional information about cases and deaths, as well as information about the health of our healthcare system in Arizona. The dashboard now has case counts broken down by zip code and more detailed demographic information about cases and deaths in our state. Data about the [...]








Social Media